Santa traveling through the multiverse – Captured in Austin, Texas – Dec. 25, 2019 (photo credit: SurfingTheUniverse.com)
20200513W Santa Cruz, CA: I spent last Christmas at my brother’s place in Austin, Texas. In walking around the neighborhood, I saw this Santa decoration. Looking at the looped version of the photo, I notice the periodic nature of the propellers and the beat of distortion. The distortion beats stimulate my imagination about how it might look to see someone traveling through the multiverse. The propellers represent for me the power that repeated habits and continuous focus can have, and how this is the power of free will which enables me to travel inter-dimensionally from one reality to another. Or at least that is how it feels and makes sense to me.
Meanwhile, in Hong Kong, protestors were going to the shopping malls not to buy presents, but to protest for human rights.
Hong Kong protesters in Sha Tin shopping mall – Hong Kong – Dec. 25, 2019 (photo credit: REUTERS/Lucy Nicholson)
I find it interesting to notice that this scene, which shows protestors wearing masks, looks normal in the post-pandemic world. At the time, mask wearing was illegal. Today, not wearing masks is illegal in some places. It’s easy to imagine a current day in which those in Hong Kong are still in the shopping mall wearing masks, and yet there is no pandemic. It is interesting to notice how some things remain constant in the timeline we experience, even if the meaning of that constant thing is different.
From Ang Ku Kueh Girl and Friend’s Chinese New Year sticker pack
20200512T Santa Cruz, CA: In this post, I’ll be discussing the origins of the coronavirus known as SARS-CoV-2 in the different sets of universes around us. Some of these universes will match the official view and some of these universes will align with conspiracy theories. Most of these universes will interfere with one another and have overlapping characteristics.
The first statement out of China was that SARS-CoV-2 was believed to have originated at a wet market in Wuhan, a large city in Hubei Province, China. Many of the early cases of COVID-19, the disease caused by SARS-CoV-2, were found in individuals who shopped at Huanan Seafood Wholesale Market. The market was closed on Jan 1, 2020, and any evidence of origin was believed to have been destroyed. A few days ago, a WHO scientist Dr. Peter Ben Embarek stated that samples taken from the wet market show that the market likely played a role in the COVID-19 outbreak. Specifically, he stated:
The market played a role in the event, that’s clear. But what role we don’t know. Whether it was the source or amplifying setting or just a coincidence that some cases were detected in and around that market,” said Dr Peter Ben Embarek in a press briefing.
Notice how this statement does not limit us to universes in which SARS-CoV-2 originated in the wet market, but also includes universes where it amplified the spread of COVID-19 and also universes in which it played no role and was only coincidentally connected.
The main unofficial and so-called conspiracy theory is that SARS-CoV-2 originated in the Wuhan Biolab not far from the wet market. This theory is circumstantial based mainly on the fact that the biolab does perform research on bat coronaviruses. This theory has two sub-theories – one in which the virus is a bioweapon and one in which it is a natural virus. There are also two overlapping sub-theories – one in which the virus was intentionally released and one in which it was accidentally released. The accidentally released theory can be further divided into one in which a lab worker is accidentally infected and one in which samples are improperly discarded.
If we assume that there is a set of universes for each of these theories and sub-theories, then the reality we see will likely be an interference pattern of these different sets of universes until one set reveals itself.
Let’s make the hypothesis/assumption that sets of universes that are in conflict will repel each other and sets of universes that are congruent will attract one another. We can begin to see a set of universes that fit together with the following features:
The Huanan Seafood Wholesale Market, a wet market, played a role in the outbreak.
The Wuhan Institute of Virology (WIV), a Biosafety Level 4 Laboratory, played a role in the outbreak.
SARS-CoV-2 was a coronavirus being studied at WIV.
SARS-CoV-2 found a way from WIV to individuals at the wet market, which was the first identified outbreak.
There are also universes where the WIV is not involved and SARS-CoV-2 is found to have come from livestock sold at the wet market. However, the future in which this is true does not appear to be sending any indications to the present that are detectible. It doesn’t fit in well with the other universes. If SARS-CoV-2 is found in live animals, it is most likely in bats not local to the Wuhan area and most likely bats from which virus samples had been collected by lab workers at WIV.
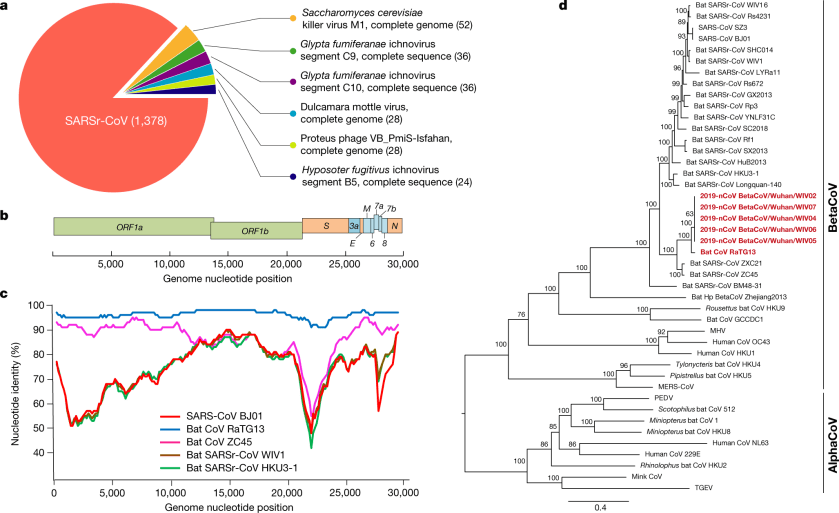
Since the SARS-CoV-2 coronavirus has been sequenced, two other coronavirus sequences have been released. The first one released is labeled RaTG13, from a sample collected in 2013 in the Yunnan province. Comparison between RaTG13 (MN996532.1) and SARS–CoV–2-Wuhan-Hu1 (MN908947.3) show that they had a most recent common ancestor estimated at 50 years ago. The second one released is labeled RmYN02, which is shown to have a most recent common ancestor estimated at 35 years ago. Neither one of these is likely to be the natural ancestor of the virus, due to the number of mutations between each and SARS-CoV-2.
Full-length genome sequences were obtained from five patients at an early stage of the outbreak. The sequences are almost identical and share 79.6% sequence identity to SARS-CoV. Furthermore, we show that 2019-nCoV is 96% identical at the whole-genome level to a bat coronavirus.
This second one I wish was explained more in how the “then found” occurred.
We then found that a short region of RNA-dependent RNA polymerase (RdRp) from a bat coronavirus (BatCoV RaTG13)—which was previously detected in Rhinolophus affinis from Yunnan province—showed high sequence identity to 2019-nCoV.
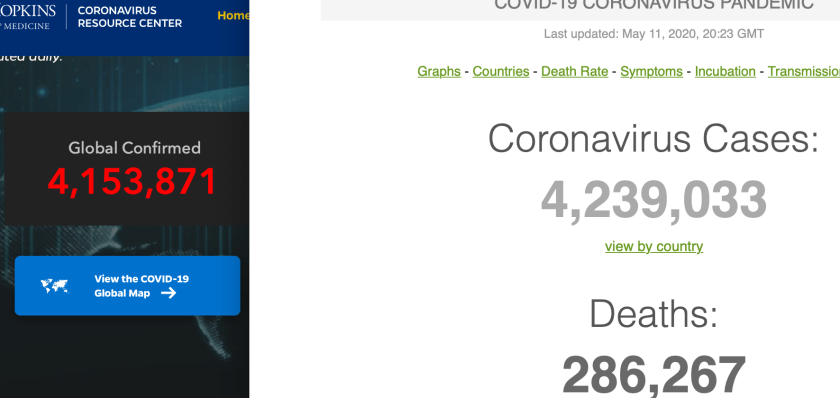
Screenshot of two coronavirus trackers on May 11, 2020, 20:23 GMT that average out to 4,196,452 – which is close to the 2^22=4,194,304 which represents a doubling of official cases every 8 days since November 17, 2019
In 20200507h Day 128: About 8 day average confirmed COVID-19 case doubling time since first case Nov 17, 2019, I noted that assuming a first case of COVID-19 on November 17, 2019, if confirmed cases had doubled every 8 days, then today we would have 4,194,304 cases. Well, an hour ago I took a screenshot of the two coronavirus trackers and the average of the two is 4,196,452. Due to the social distancing measures now in place throughout the world, to the seasonal nature of coronavirus infections, and to the now ramped up testing, we are no longer increasing cases at an 8-day doubling rate.
If our confirmed cases had exactly doubled every 8 days, here is how the cases would have grown, with comparison to confirmed cases reported:
According to the government data seen by the Post, a 55 year-old from Hubei province could have been the first person to have contracted Covid-19 on November 17.
From that date onwards, one to five new cases were reported each day. By December 15, the total number of infections stood at 27 – the first double-digit daily rise was reported on December 17 – and by December 20, the total number of confirmed cases had reached 60.
On December 27, Zhang Jixian, a doctor from Hubei Provincial Hospital of Integrated Chinese and Western Medicine, told China’s health authorities that the disease was caused by a new coronavirus. By that date, more than 180 people had been infected, though doctors might not have been aware of all of them at the time.
By the final day of 2019, the number of confirmed cases had risen to 266, On the first day of 2020 it stood at 381.
The graduates, 97% of whom were in South Korea, had completed an 8-month theology program that covers the Bible, with emphasis on the prophecies from the book of Revelation. The graduation ceremony was held on November 10, 2019.
From the article:
Of course it is incredible enough to see 100,000 students graduating from a single denomination; however, what is more shocking is that Shincheonji — which is teaching the fulfillment of Revelation and has been growing at an incredibly rapid pace since 1984 is labeled as a “cult” by the Christian world of the Republic of Korea especially through the CCK (Christian Council of Korea).
The growth of Shincheonji is expected to grow exponentially after the graduation. With the evangelism rate of the graduates being over 100%, currently there are 200,000 plus students that are enrolled in the theology program. If Shincheonji continues to grow at this pace, then within 3 years it will reach a million congregation members, and the status quo of the religious world will change.
On the day prior, there was another article on prnewswire.com:
Shincheonji Church of Jesus, the Temple of the Tabernacle of the Testimony (SCJ) is calling for the resignation of the President of the Christian Council of Korea (CCK) Pastor Jun Kwang-hoon as well for the CCK to be disbanded following controversial comments made by Pastor Jun.
A representative of Shincheonji Church of Jesus said, “President Jun Kwang-hoon claims that he has been anointed, and even asserting that the entire country of South Korea centers around him, and that he will kill God if things do not go his way.” He also explained, “Such assertions expose his heretic beliefs that use religion for power and oppose God. The CCK – a political organization masked under religion – must be shut down immediately.”
On Feb 26, 2020, an article in businessinsider.com had this interesting quote which mentions rumors about a virus began circulating in November:
“Rumours about a virus began to circulate in November but no one took them seriously,” an anonymous 28-year-old kindergarten teacher who belongs to Shincheonji told the Post. “I was in Wuhan in December when our church suspended all gatherings as soon as we learned about [the coronavirus].”
The kindergarten teacher wouldn’t comment on whether any Shincheonji members from Wuhan had traveled to South Korea recently but also insisted that they had nothing to do with the mass COVID-19 cases that have erupted there.
“I don’t think the virus came from us because none of our brothers and sisters in Wuhan have been infected,” she told the Post. “I don’t know about members in other places but at least we are clean. None of us have reported sick. There are so many Chinese traveling to South Korea, it’s quite unfair to pin [the disease] on us.”
Adding the common cold treatment of Zinc and Vitamin C with Schweppes tonic water is a so called “fake” treatment for COVID-19. Reference: Tweet by @RockNRoll761 on Apr 9
Hydroxychloroquine has been a controversial treatment for COVID-19, at least since President Trump mentioned it as a potential treatment, along with Zinc, at a daily briefing. Various attempts to show the efficacy of Hydroxychloroquine have shown mixed results. Those who believe Hydroxychloroquine is harmful point to studies showing apparent side effects with no benefits. Those who believe Hydroxychloroquine could be helpful, claim that in order to be effective, it must be administered early and with Zinc. This paper attempts to address the question of whether the addition of Zinc makes a difference. The results shown in the paper indicate that Zinc is helpful. From the Results section:
The addition of zinc sulfate did not impact the length of hospitalization, duration of ventilation, or ICU duration. In univariate analyses, zinc sulfate
increased the frequency of patients being discharged home, and decreased the need for ventilation, admission to the ICU, and mortality or transfer to hospice for patients who were never admitted to the ICU. After adjusting for the time at which zinc sulfate was added to our protocol, an increased frequency of being discharged home (OR 1.53, 95% CI 1.12-2.09) reduction in mortality or transfer to hospice remained significant (OR 0.449, 95% CI 0.271-0.744).
The conclusion of the paper:
This study provides the first in vivo evidence that zinc sulfate in combination with hydroxychloroquine may play a role in therapeutic management for COVID-19.
Here are some quotes that I found of interest from the paper, along with some of my thoughts:
The U.S. Food and Drug Administration authorized the emergency use of hydroxychloroquine for the treatment of COVID-19 with or without azithromycin.
I’m curious where Zinc fit into the authorization – and if dosage levels were mentioned.
Chloroquine analogues are weak bases that concentrate within acidic endosomes and lysosomes. Once intracellular, chloroquine analogues become protonated and increase pH resulting in prevention of endosomal trafficking, dysfunctional cellular enzymes, and impaired protein synthesis [7].
This inhibits viral replication through interference with endosome-mediated viral entry or late transport of the enveloped virus. Further, this results in interference with the terminal glycosylation of ACE2 receptor expression which prevents SARS-CoV-2 receptor binding and spread of infection [8].
[7] is a 2003 paper written (in The Lancet Infectious Diseases) during the initial SARS epidemic by Savarino et. al. entitled Effects of chloroquine on viral infections: an old drug against today’s diseases.
[8] is a 2005 paper written (in Virology Journal) just after the initial SARS epidemic by Vincent et al. entitled Chloroquine is a potent inhibitor of SARS coronavirus infection and spread.
For COVID-19, hydroxychloroquine (a hydroxy-derivative of chloroquine) has been proposed to be used instead of chloroquine. Recently, it has been shown to have 3x higher cytotoxic potential in vitro against SARS-CoV-2 compared to chloroquine [9].
[9] is a 2020 paper (written in Clinical Infectious Diseases) by Yao et. al. entitled The Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2).
A 2010 paper (written in PLOS Pathogens) by the Velthuis et. al. entitled Zn2+Inhibits Coronavirus and Arterivirus RNA Polymerase Activity in Vitro and Zinc Ionophores Block the Replication of These Viruses in Cell Culture. The title pretty much says it all.
The idea behind combining Hydroxychloroquine with Zinc is based on the difficulty of achieving a high enough intracellular concentration of Zinc without a zinc ionophore, such as chloroquine. (Reference: Xue et. al. 2014 paper in PLoS one entitled Chloroquine is a zinc ionophore)
Regarding the main finding of this paper:
The main finding of this study is that after adjusting for the timing of zinc therapy, we found that the addition of zinc sulfate to hydroxychloroquine and azithromycin was found to associate with a decrease in mortality or transition to hospice among patients who did not require ICU level of care, but this association was not significant in patients who were treated in the ICU.
Our findings suggest a potential therapeutic synergistic mechanism of zinc sulfate with hydroxychloroquine, if used early on in presentation with COVID-19.
The authors identified a number of limitations of their study and ended with:
In light of these limitations, this study should not be used to guide clinical practice. Rather, our observations support the initiation of future randomized clinical trials investigating zinc sulfate against COVID-19.